

The Lambano Sanctuary.
As part of our CSR initiative and in line with our values, we at the JHB Eye Hospital strive to help our community wherever we can.
We recently donated 4 beds and a baby crib to support this wonderful organisation – The Lambano Sanctuary.
Lambano Sanctuary is an accredited HPCA organisation that provides care to children with life-limiting and life-threatening illnesses.
The organisation was established in 2001 and has grown into four homes that permanently care for children between the ages of 9 and 19.
Their first Paediatric Medical Stepdown Facility was opened in 2009. Lambano’s aim is to care for children and provide social support to families.
To read more about Lambano Sanctuary please visit their Facebook page:
https://www.facebook.com/lambanosanctuary/
Michael
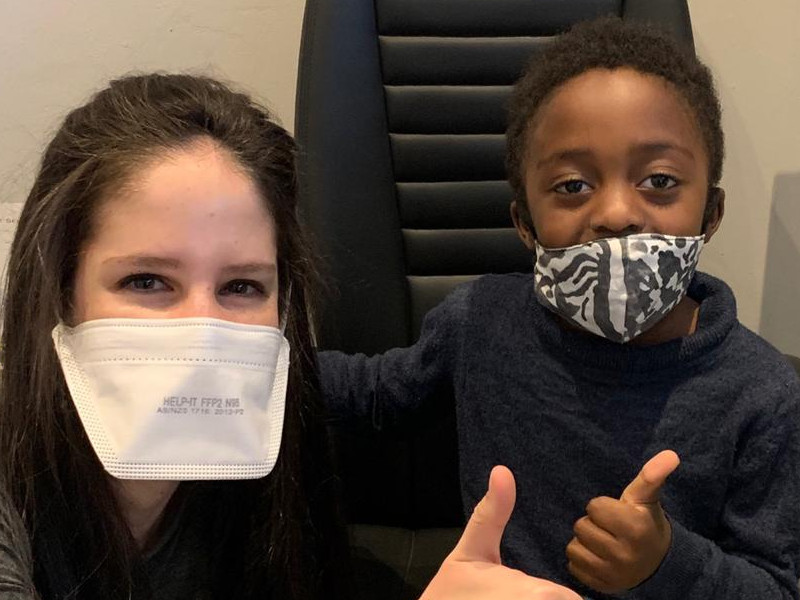
As part of our CSR initiative, we at the JHB Eye Hospital strive to help our community through the support of all our doctors, by assisting with restoring the gift sight to members of the community who need our help.
Meet Michael, a wonderful strong and independent six-year-old. He underwent surgery by Dr Esra to remove a large conjunctival cyst that had been growing under his left eye for three months. It was becoming uncomfortable to bare and was and altering his appearance significantly. Due to his age and the large size of the cyst, the removal required surgery with a general anaesthetic in theatre at the Johannesburg Eye Hospital. The procedure was a huge success. Michael and his family are very thankful to all the stakeholders that were involved with his surgery at the JHB Eye Hospital.

The causes of visual impairment in children in a school for the blind in Johannesburg
Childhood blindness in South Africa
The causes of visual impairment in children in a school for the blind in Johannesburg
N Esra MBBCh, FC (Ophth)SA, MMed; Registrar*
I Mayet MBChB, FC(Ophth)SA, FRC(Ophth); Head of Department St John Eye Hospital*
* Department of Ophthalmology, University of the Witwatersrand, Johannesburg, South Africa; and St John Eye Hospital, Johannesburg, South Africa
Corresponding author: Dr N Esra, PO Box 1128 Highlands North, Gauteng, South Africa, 2037; email: [email protected]
Abstract
Background: More than 1.4 million children are blind worldwide. The significance lies in the social, emotional and economic implications of childhood visual impairment, which are endured throughout a lifetime of ‘blind years’. Information regarding the epidemiology and risk factors relating to childhood visual impairment is essential for the development and implementation of targeted interventions.
Objectives: To identify the causes of childhood blindness in a school for the blind in Johannesburg, South Africa, as a representation of trends in our urban population.
Methods: All learners attending a school for the blind in Johannesburg were evaluated. Information obtained was recorded using the World Health Organization’s programme for the prevention of blindness (WHO/PBL) method and reporting form.
Results: A total of 189 learners were examined, of which 110 (59%) had severe visual impairment or blindness. The major affected anatomical sites were the retina (42%), whole globe (16%), optic nerve (10%), cornea (8%), uvea (6%) and lens (5%). Retinopathy of prematurity was the most common retinal condition (n=26, 14%). Hereditary conditions were responsible for 28% of visual impairment in learners. Aetiology was indeterminate in 41% of learners. Avoidable causes accounted for 29% of learners.
Conclusion: There has been a change in the disease pattern of childhood blindness in this study population, when compared to the findings of a nationwide study conducted in 1996. While many advances have been made regarding immunisation, vitamin supplementation and ophthalmic management of paediatric cataracts, the implementation of further measures are still required in order to overcome avoidable causes of childhood visual impairment.
Keywords: ophthalmology, paediatrics, South Africa, prevention, public health
Funding: Transportation of learners from Sibonile School to St John Eye Hospital, for examination, was paid for by Retina South Africa, a non-profit organisation.
Conflict of interest: Neither of the authors have any proprietary interests or conflicts of interest related to this submission.
Introduction
It has been estimated that 1.4 million children are blind globally, three-quarters of whom are from developing countries.1 The World Health Organization’s (WHO) Vision 20/20 – The Right to Sight Programme has highlighted the importance of the management and control of visual impairment in childhood. This is for a number of a reasons: 1) individuals who are born blind or become blind during their childhood endure a lifetime of ‘blind years’ with their accompanying social, emotional and economic implications; 2) many causes of visual impairment in childhood are preventable or curable, particularly in developing countries where over 30% of childhood blindness has been found to be avoidable; and 3) several of these causes also lead to child mortality and therefore their management is associated with improved child survival.2
In order for the implementation of 27
targeted interventions, more information is needed regarding the epidemiology and risk factors relating to childhood visual impairment.3 These are affected by a variety of factors including, age, geographic location, level of socio-economic development and health care accessibility.4 Genetic or hereditary diseases are the main cause of childhood blindness in developed countries.5 In developing countries, the main aetiologies have been found to be related to infections (congenital rubella or acquired measles infection) or nutritional deficiencies (vitamin A deficiency).5
South Africa (SA) has been classified as an upper middle-income economy, the largest in Africa.6 Despite this, poverty and inequality continue to soar.6 Since the establishment of democracy, unemployment has been exceptionally high, worsening between 1994 and 2003, thereby altering the population’s access to health care.6 Despite the disparity in access to health care in SA, there have been major improvements in the last 21 years with regard to measles immunisation, vitamin A supplementation, and antenatal and neonatal care.
The most recent data available for the causes of childhood blindness in SA were collected in a nationwide study of blind schools in 1996, which found that 39% of childhood visual impairment was avoidable.7 Retinal disease featured prominently, with dystrophies and albinism accounting for the majority of cases in this disease spectrum. Retinopathy of prematurity (ROP) was found to be an emerging and preventable aetiology of blindness in white and Indian communities.7 Twelve per cent of the children included in this study had normal vision or mild visual impairment and the need for possible integration of these children into mainstream schooling was identified.7
Objectives
The aim of this study was to identify the causes of childhood blindness in a school for the blind in Johannesburg, South Africa, as a representation of trends in our urban population, in order to inform health policy decision-making.
Methods
Patient selection
This was a cross-sectional study of all 189 learners attending Sibonile School in the south of Johannesburg, South Africa, that caters for the education of blind and partially sighted learners, including those with multiple disabilities.
Data acquisition
The 189 learners enrolled in the school were examined by an ophthalmic registrar at St John Eye Hospital from 1 September 2017 to 15 September 2017, with assessments confirmed by two ophthalmic consultants.
Each learner was examined in the presence of his or her teacher. Data were extracted from previous medical records, where available. Uni-ocular visual acuity was measured, where possible, using Snellen charts and Sheridan-Gardner test cards. A torch or slit lamp were used to examine the anterior segment. An indirect ophthalmoscope was used for posterior segment evaluation, following mydriasis. B-scan ultrasonography was performed when indicated. Examinations were conducted using the World Health Organization’s programme for the prevention of blindness (WHO/ PBL) method and reporting form, a standardised assessment tool for reporting of the causes of visual loss.8
Visual impairment was documented according to the category of visual impairment, graded 0 to 5, and using the anatomical and aetiological classifications in the form.
Where indicated, learners were scheduled for further assessment, surgery and refraction.
Ethical approval was obtained from the University of the Witwatersrand Human Research Ethics Committee (clearance number M170211) and from the both the Hospital Management and Department of Education.
Results were entered onto an Excel spreadsheet (2011, Microsoft, USA). With the consult of a biostatistician, data analysis was carried out using STATA® (v 12.0). These results were documented and displayed graphically by means of tables.
Results
A total of 189 learners were included in the study. There were 121 (64%) males, and 68 (36%) females, all of black ethnicity. The mean age of the learners was 11.3 years (standard deviation 3.2 years) with a range of 5–20 years. Additional disabilities, including mental retardation, physical handicap and epilepsy were found in 37 (20%) cases.
Categories of visual impairment
The distribution of visual impairment according to the WHO categories are shown in Table I. Twenty-seven learners (15%) were found to have mild or no visual impairment (equal to 6/18 or better), 47 (26%) moderate visual impairment (6/18– 6/60) and 110 (59%) learners were blind (less than 3/60). Learners who were classified blind had 3/60 to light perception in 43% (n=80) and no light perception in 16% (n=30). Due to multiple disabilities, the degree of visual impairment could not be assessed in five learners.
Anatomical site of visual abnormality
The anatomical sites of abnormality in the learners are shown in Table II.
| Table II: Anatomical sites of abnormality resulting in visual impairment | |
| Site | n (%) |
| Retina | 79 (42) |
| Whole globe | 30 (16) |
| Normal globe | 25 (13) |
| Optic nerve | 18 (10) |
| Cornea | 16 (8) |
| Uvea | 12 (6) |
| Lens | 9 (5) |
To read more in this exciting research please click in the link below

Dry Eye Disease
Dry Eye
By Lizelle Dorfling-Smith
Optometrist
B.Optom (RAU) CAS (NECO)
1. How Common is this condition
According to a National Health and Wellness Survey done in 2013, it was found that approximately 6 million people reported to experience DED (Dry Eye Disease) symptoms. Although, these mentioned people, had not been formally diagnosed with DED. (1)
It also happens very frequently that when a DED diagnosis is made, the clinicians often underestimate the severity. One study found that more than 54% of patients over 65 years of age and 43% of female patients had their dry eye severity very underestimated by their clinician. (2) This is without a doubt a condition that is very prevalent but not enough in depth attention is given to improving the symptoms in the long term.
A. What does a tear layer consist of and how does it function?
Your tear layer consists of 3 parts:
i. Sticky Mucin Layer
ii. Aqueous Layer
iii. Lipid Layer
These 3 layers work together to provide a stable tear layer. As a unit these three layers protect your eye from infections, foreign particles and create a healthy surface. This tear layer also provides an optically optimal surface to bend light for a clear image. If any of these 3 layers are deficient or lacking, you can have a dry eye and experience some dry eye symptoms. The degrees of these symptoms are dependent on how much any of these 3 layers are affected.
B. A breakdown of these layers can be caused by a variety of factors including:
i. Environment
Very windy, dry conditions as well as a low humidity can aggravate dry eye symptoms. This also includes environments with air-conditioners and extended periods of computer work.
ii. Age
Women are diagnosed much earlier in age with with Dry Eye Disease (DED) than men. (3)
iii. Gender
Gender is one of the greatest risk factors for dry eyes. This is because of varies factors such as auto-immune diseases over the age of 50, (3) as well as the fact that woman are more likely to experience dry eye symptoms due to hormonal changes during pregnancy and menopause.
iv. Medical Conditions
As mentioned above, Auto-immune diseases are the most related to dry Eye Disease.
v. Medication
2. COMMON SYMPTOMS
Dry Eye can present with all or some of the following symptoms:
i. A sandy or gritty feeling
ii. Sore, red eyes
iii. Uncomfortable or painful sensation
iv. A feeling of itchiness or burning
v. Intermittent blurry vision
vi. Watery eyes, as if you are crying. Watery eyes often means that you are producing poor quality tears causing it to evaporate too quickly hence forming more and more tears because of the underlying dryness still present.
- EPIDEMIOLOGY
A recent survey had revealed that 66% of Ophthalmologists report that patients present with screen related eye problems, and 88% point to smartphone use as the cause of rising a DED (Dry Eye Disease) prevalence.(4) Hand held electronic devices are also now recognised as a risk factor for DED because it reduce the rate of blinking and it causes the tear film to evaporate faster. (5)
The “cost”of managing DED by Ophthalmologist has also shown a great economical impact all over the world, as shown by a study done by Mc Donald et al. in 2016. (6)
It showed the cost of managing a 1000 DED patients to be around $270 000 in France, $1.1 Million in the U.K. and $782,673 in the US. They suggested that the cost of DED is likely higher due to the “widespread use of over-the-counter artificial tears” by patients with dry eye symptoms. This is astounding numbers. The question remains if we are approaching this condition in the correct way.
4. Diagnosis
Firstly there are very helpful questionnaires that can help to establish if there are dry eyes symptoms experienced. Examples are the DEQ-5 and OSDI Questionnaires that can also be downloaded as an app.
Secondly a thorough eye examination will be done to screen for any dry eye signs.
If both positive signs and symptoms are detected, a proper dry -eye-workup needs to be done in order to diagnose the type of dry eye:
a. Evaporative Dry Eye
The most common type of dry eye associated with Meibomian gland dysfunction (MGD) and Blepharitis.
b. Aqueous Deficient Dry Eye
This one is less common and usually associated with medical conditions and auto-immune diseases.
c. Combination of the above.
More than one third of patients show a combination of Evaporative and Aqueous deficient Dry Eye. (7)
Determining what kind of dry eye you have is extremely important in deciding what the treatment plan needs to be. Dry Eye treatment is a more intricate process than what we think.
5. Treatment
Simply adding artificial tears and then moving to punctual plugs are just not enough to show a positive improvement in Dry Eye in the long term. These only treat the symptoms but not the actual cause of the Dry Eye.
There needs to be a long term plan and not just a once of “solution” that will hopefully do the trick.
Especially with MGD causing evaporative Dry Eye, the patient also needs to get involved in the treatment and management of this condition over a period of weeks and learn some good eyelid hygiene habits. Evaporative Dry Eye is a very common cause of Dry Eye and the patient needs to come for weekly visits where the eyelids can be treated for greater long term relief and success
Patients needs to be co-managed with the Clinician over a period of weeks after the workup was done to establish the type of dry eye and the severity of it.
Every treatment plan needs to be worked out for each patient individually, as no one patient is the same and neither is their dry eye condition.
For this reason the treatment of Dry Eye has moved to a more in depth analysis, diagnostic and treatment regimen in the form of Dry Eye Clinics.
These Dry Eye Clinics are only available at certain Clinician & Optometrist practices.
You are welcome to leave us an enquiry regarding these Dry Eye Clinics for more information.
REFERENCES
1. Farrand KF, Fridman M, Stillman IO, Schaumberg DA. Prevalence of Diagnosed Dry Eye Disease in the United States Among Adults Aged 18 Years and Older. Am J Ophthalmol 2017;182:90-8.
2. Asbell PA, Spiegel S. Ophthalmologist perceptions regarding treatment of moderate-to-severe dry eye: results of a physician survey. Eye Contact Lens 2010;36(1):33-8.
3. Dalton M. Understanding prevalence, demographics of dry eye disease. Ophthalmology Times July 2019. https://www.ophthalmologytimes.com/view/understanding-prevalence-demographics-dry-eye-disease
4. Hoffman M. Survey Data Reveals Major Concern About Screen Use, Chronic Dry Eye. MD Magazine,2018.
5. Moon JH, Kim KW, Moon NJ. Smartphone use is a risk factor for pediatric dry eye disease according to region and age: a case control study. BMC Ophthalmol 2016;16(1):188
6. McDonald M, Patel DA, Keith MS, Snedecor SJ. Economic and Humsnistic Burden of Dry Eye Disease in Europe, North America, and Asia: A Systematic Literature Review. Ocul Surf 2016;14(2):144-67
7. Lemp MA, Crews LA, Bron AJ, et al. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea 2012;31(5):472-8

How would I know I have retinal disease?
How would I know I have retinal disease?
by Dr Annalien Steyn
Retinal disease is extremely important to identify early, as irreversible vision loss can occur if certain conditions are not picked up early and treated. So how will you know that you may have a retinal disease or problem?
Flashes and floaters
A flash of light or lightning streak may be seen inside the eye when the vitreous gel (jelly like substance filling the eye) pulls on the retina. If you suddenly experience new flashes of light, it is important to see an ophthalmologist urgently as this could mean that the retina has torn.
Floaters are small opaque items, like clouds, moving in and out of your vision. They can take on many shapes like dots, clumps, lines and even cobwebs. These floaters seem to be in front of the eye, but they are actually floating around in the vitreous. Floaters may be a normal aging process as the vitreous shrinks and forms strands and clumps in the eye, or when a posterior vitreous detachment occurs- meaning the vitreous gel pulls away from the wall of the eye. New onset of floaters should prompt you to see an ophthalmologist as it may indicate a torn retina.
Defects in one area of vision
This is often described as a curtain hanging over the eye. It may start in a small area of the eye and them become bigger. You will have no vision where this “curtain” hangs over the eye. This is an emergency as it may be a retinal detachment and you should see an ophthalmologist urgently.
Loss of vision
A sudden loss of vision in one, or even both eyes, can also be seen in retinal disease. With sudden vision loss, you can often pinpoint the exact time at which you lost vision. Many conditions can cause this and it is important to see an ophthalmologist urgently to find the reason as it may be sight threatening.
Distorted vision
The scientific name for this is metamorphopsia and this term is used when straight lines look wavy. You can close one eye at a time and look at any straight line to see if it remains straight or becomes wavy at any point. Distorted vision most commonly points to a macular problem, the most common of which is age related macular degeneration. If you develop distorted vision, it is important to see an ophthalmologist to find the reason for visual distortion and possible treatment options.

Re-opening of the Medwedge Stepdown Facility

Our Medwedge Stepdown Facility has welcomed its first patients back since South Africa’s lockdown started in March this year. We are ready to ensure a safe and secure environment for patients to achieve a healthy recovery with optimal outcomes.
We offer each patient an individual care plan to assist with each patient’s individual needs.
Our current in-house patients include neurological trauma and orthopaedic recoveries from our feeder hospitals including Netcare Olivedale, Life Wilgeheuwel and Netcare Rosebank.
Our Medwedge Stepdown facility is a sub-acute licenced facility with 37 beds available for patients who need comprehensive medical care and rehabilitation after a surgical procedure or illness. We are contracted to medical aids and form a part of the greater NHN Hospital group.
The facility focuses on post-surgery from the following disciplines: General Medical – which includes all non-infectious medical patients, Orthopaedic, Stroke recovery and Cardiac patients.
Additional specialty services include Physiotherapy, Speech Therapy, Occupational Therapy and a General practitioner.

Hulp dringend nodig vir klein Leonel
Dinsdag 2 Junie is ‘n dag wat die ouers van die 4-jarige Leonel Riekert van Parys nie sal vergeet nie.
Leonel het geval terwyl sy ‘n skêr in haar handjies gehou het. Die skêr het haar linkeroog en wang gepenetreer.
Die besering in haar ogie was egter baie groter as wat aanvanklik verwag is.

Oogspesialis, dr Corné Gouws het die wond Woensdagoggend toegemaak, maar vandag, Donderdag 4 Junie, is daar met die ondersoek gesien dat die retina los is en ‘n vitreo-retinale spesialis in Johannesburg dringend die herstel daarvan moet hanteer om die visie in klein Leonel se ogie te probeer red.
Die kostes van die herstel van die operasie word geraam op ongeveer R60 000. Die eerste operasie wat Leonel moes ondergaan het reeds R20 760 gekos.
Die gesin het nie ‘n mediese fonds nie, en die staat kan nie tans so ‘n delikate operasie hanteer nie.

Leonel se ouers sien môre die vitreo-retinale spesialis, in Johannesburg in die hoop om hul dogtertjie se sig te red.
As jy op enige manier hierdie gesin kan ondersteun met ‘n bydrae om die operasie moontlik te maak, kan jy ‘n elektroniese bydrae maak in die prokureurs-trustrekening waar alle fondse vir Leonel se operasie deur prokureur Stefan Scheepers geadministreer sal word.
Die bankbesonderhede vir die trustrekening is: Stefan Scheepers Ingelyf, FNB Trustrekening takkode 230736, rekeningnommer 62703192394. Gebruik asseblief die verwysing Leonel Riekert.
Source: https://parysgazette.co.za/38452/hulp-dringend-nodig-vir-klein-leonel/

Leonel (4) ondergaan delikate operasie na skêr-ongeluk
Leonel is Dinsdag in die Johannesburgse Ooghospitaal deur dr. Bernard Wolff geopereer waar gesien is wat die omvang van die skade aan haar ogie is, wat ernstig beseer is na ‘n fratsongeluk Dinsdag, 2 Junie toe sy met ’n skêr wat sy in haar handjies gehou het, geval het.
Hoewel oogspesialis, dr. Corné Gouws, verlede Woensdag die wond toegemaak het, is daar Donderdag, 4 Junie met die ondersoek gesien dat Leonel se retina weens die besering los is, en is sy na dr. Wolff, ‘n vitreo-retinale spesialis, verwys.
Die gesin het nie ’n mediese fonds nie en die staat doen tans nie sulke delikate operasies soos wat Leonel dringend moes kry om haar sig, en skade aan haar oog te probeer herstel nie.
Sedert die Gazette Donderdagmiddag oor klein Leonel se fratsongeluk berig het, is ‘n trustfonds vir haar gestig wat deur prokureur Stefan Scheepers van Parys geadministreer word.
Mense van oral oor het eenvoudig net hul harte oopgemaak vir die gesin en is binne twee dae
R125 000 vir Leonel ingesamel wat genoeg was om Dinsdag se operasie te kon betaal, en te help met die opvolgoperasies en behandeling wat sy sal nodig hê.
Vir Leonel gaan dit ‘n lang pad na herstel wees, maar pak haar ouers, André en Mari, elke dag in geloof aan.
Hulle sê dat woorde nie kan beskryf hoe ongelooflik dankbaar hulle is vir elke oproep, boodskap, gebed of bydrae. Daar is eenvoudig net te veel name om te noem.
Van kunstenaars wat bereid was om Leonel se storie op hul sosiale platforms te deel, tot die Secret Saints van Vereeniging en ander organisasies en individue wat ingespring het om te help. Elke bydrae word opreg deur hierdie gesin waardeer.
Source: https://vaalweekblad.com/65142/leonel-4-ondergaan-delikate-operasie-na-sker-ongeluk/